Download and complete the Medicare Claim form. Please FAX Part B forms to.
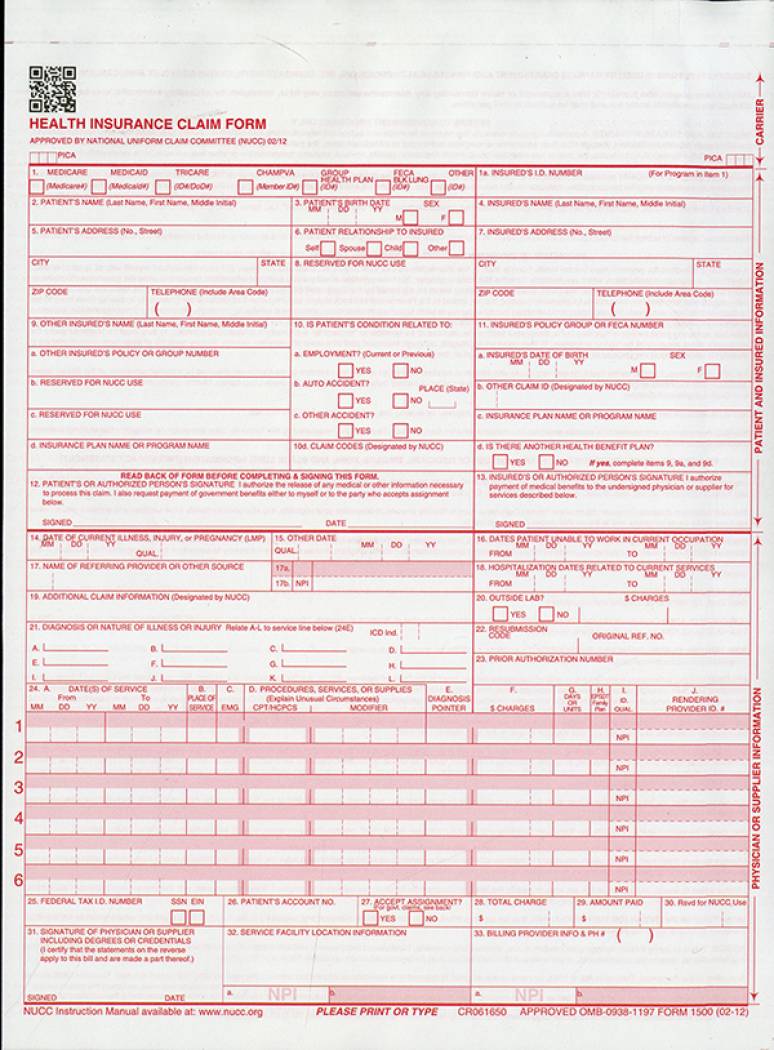
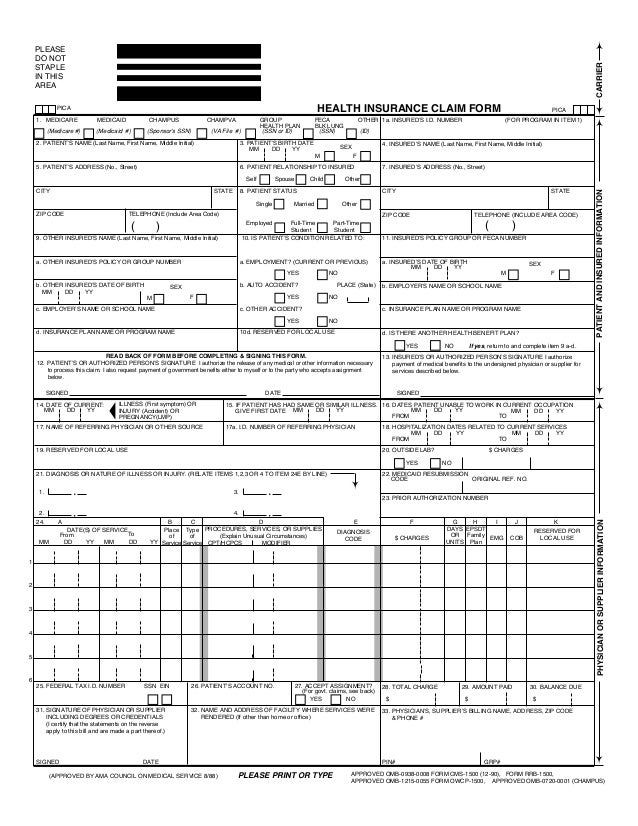 Health Insurance Claim Form Cms1500 Hosa
Health Insurance Claim Form Cms1500 Hosa
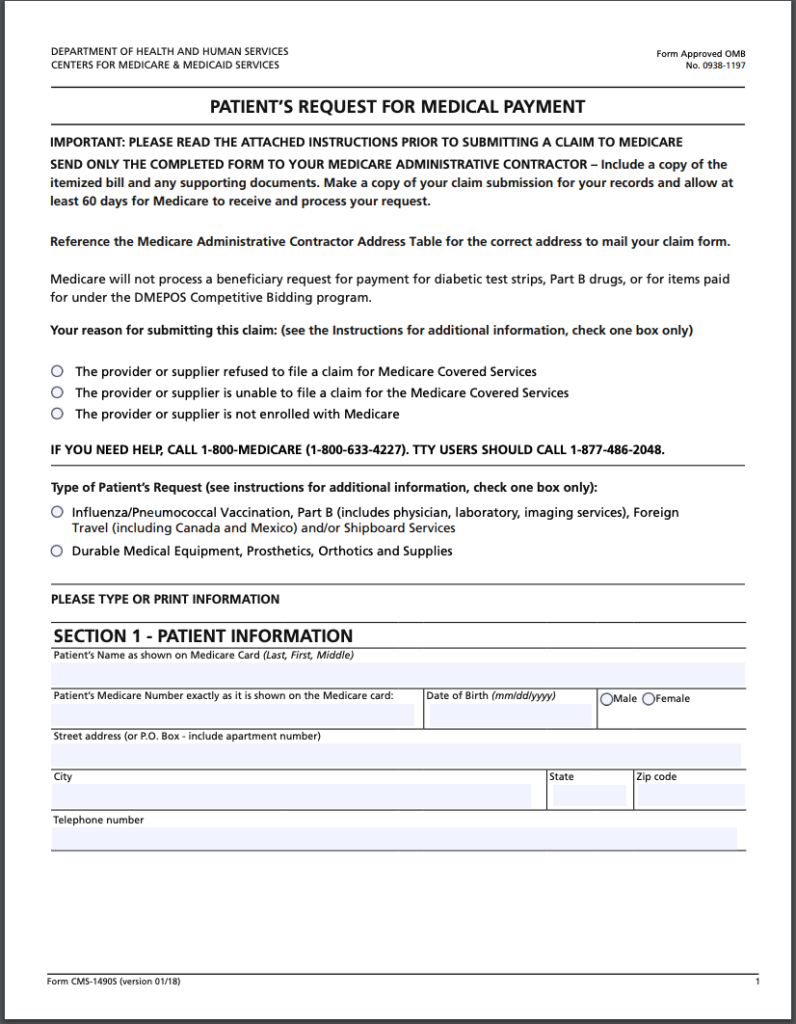
Durable Medical Equipment Prosthetics Orthotics and Supplies.
Medicare part b claim form. To find out more about how to terminate Medicare Part B or to schedule a personal interview contact us at 1-800-772-1213 TTY. This can be for a paid or unpaid account. Complete a separate form for your.
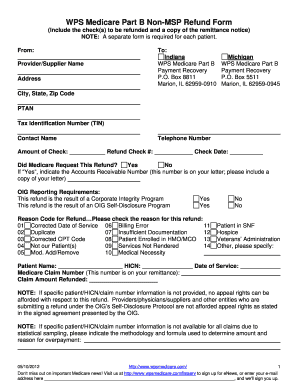
Government Printing Office at 202-512-1800. Check the first boxif your Medicare Part B premium. Providers must submit Medicare initial claims electronically unless the provider qualifies for a waiver.
I will be sending claims. For a paper claim to be considered for MSP benefits a copy of the primary payers EOB notice must be forwarded along with the claim form. It can be purchased in any version required by calling the US.
Medicare Part B which provides you with medical insurance under Medicare. If you qualify for a waiverexception under the Administrative Simplification Compliance Act to submit paper claims rather than electronic claims send MSP claims to one of the appropriate addresses below. IRMAA Medicare Part B.
SECTION 2 - Part B Premiums Claimed Please note that this reimbursement claim will not be valid without proof of payment such as Form CMS-500 Notice of Medicare Premium Due attached. This form is available both in English and Spanish. The CMS-1500 Form is the prescribed form for claims prepared and submitted by physicians or suppliers whether or not the claims are assigned.
There will be no need to file a. MEDICARE PART B REDETERMINATION AND CLERICAL ERROR REOPENING REQUEST FORM FAX to. 2018 Medicare Part B Reimbursement Differential Request Form.
Please print or write legibly when completing the account holder first and last name. The following forms are designed for Part B providers who submit claims to CGS. Youll need to complete the form during an interview with a representative of the Social Security Administration SSA by phone or in person.
Fill out the Application for Enrollment in Part B CMS-40B. Type of Bill TOB 13x. In most situations your physician other practitioner or supplier will submit your claim to Medicare if they do not you can submit a claim.
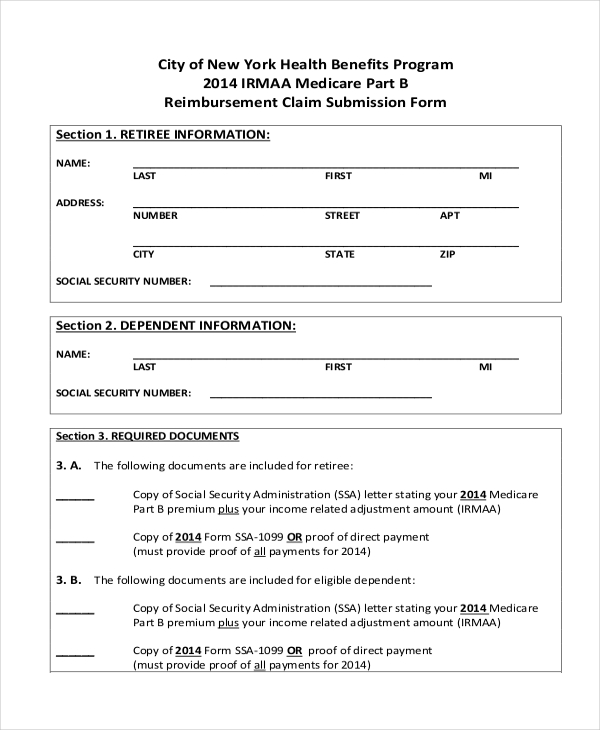
2017 Medicare Part B Reimbursement Differential Request Form. The form requires your name claim number that is your Medicare ID number as it appears on your. Submit an outpatient Part B claim containing the below information on the UB-04 claim form.
I want to sign up for Part B while Im employed or during the 8 months after employment or my employerunion coverage has ended and I need to provide employment information Request for Employment InformationCMS-L564. Before submitting a hard copy claim on the Form CMS-1500 health care professionals and suppliers must self-. You can only sign up using this form if you already have Medicare Part A Hospital Insurance.
FILLING OUT YOUR CLAIM FORM. Part B EDI Application Cahaba Government Benefit Administrators. If your answer to this question is no then you dont need to fill out this application.
Type directly into the required fields electronically then print and sign if required. How to cancel Medicare Part B The Part B cancellation process begins with downloading and printing Form CMS 1763 but dont fill it out yet. A Social Security representative will help you complete Form CMS 1763.
Medicare Claim form MS014 Use this form to claim Medicare benefits by mail or in person at a service centre. 1-888-541-3829 PLEASE COMPLETE EACH FIELD ON THE FORM TO ENSURE ACCURATE PROCESSING. This application is to sign up to get medical insurance under Medicare.
Do not complete this form for the following situations. 2020 Medicare Part B Reimbursement Differential Request Form - Information available May 2021. Be sure that this cover page with the bar code is used in your fax submission.
Or exception under the Administrative Simplification Compliance Act ASCA requirement for electronic. CMS Form 1490S Patients Request for Medical Payment is a claim form that you can use to request payment for Medicare Part B covered services CMS Form 1490S Patients Request for Medical Payment is a claim form that you can use to request payment for Medicare Part B covered services. 2019 Medicare Part B Reimbursement Differential Request Form.
CMS Medicare Learning Network MLN Special Edition SE1333 - Instructions for Implementation of Final Rule 1599-F for Part A to Part B Billing of Denied Hospital Inpatient Claims. If you do not have Adobe Reader software you can download it at no cost. Account Holder Information.
This section should be filled out according to how your Medicare Part B premiums are paid. IRMAA Medicare Part B Reimbursement. Submit one specialized reimbursement form to setup automatic reimbursement for the rest of the year.
Spouse andor covered dependents. You can also contact your nearest Social Security office. 1-800-325-0778 between Monday through Friday from 800 am 700 pm.
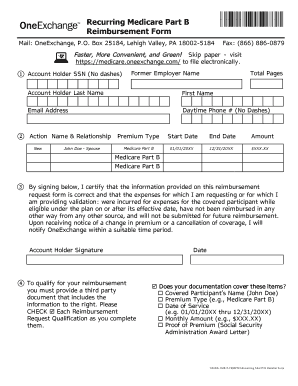
Medicare Part B Reimbursement Recurring Medicare Part B Reimbursement is for those who want to be automatically reimbursed monthly for their premiums deducted from their social security benefit check. Claims for Out-of-Pocket Expenses. All forms are in the Portable Document Format pdf.
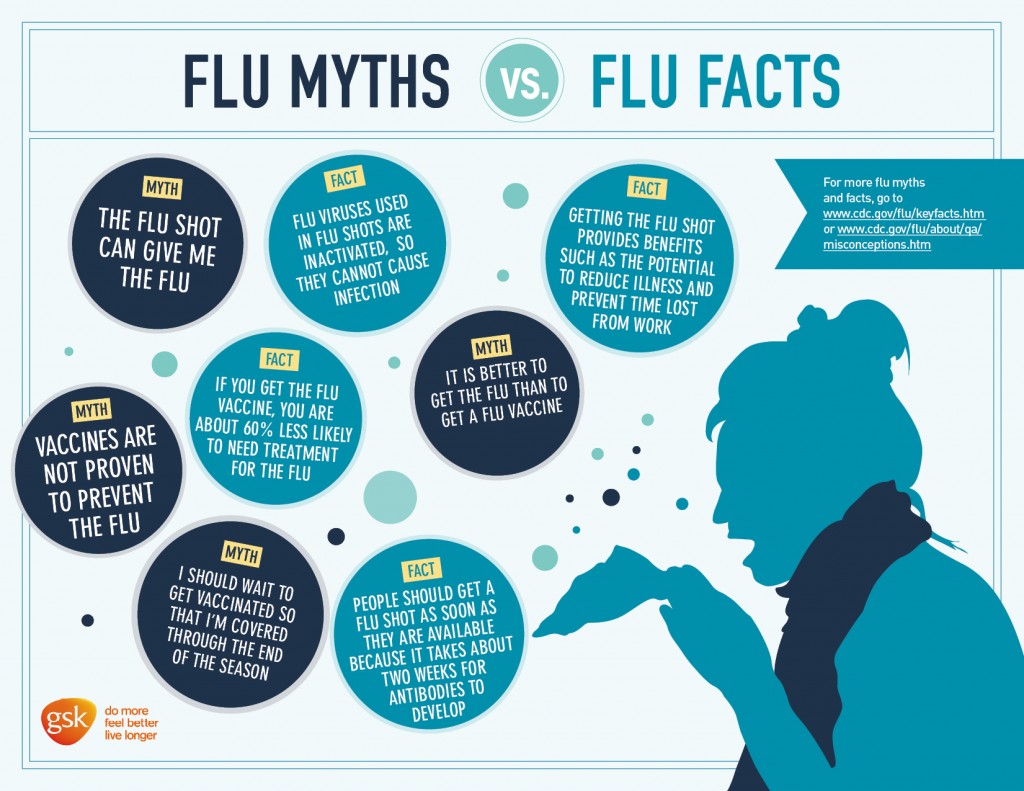
Practitioners and suppliers who administer seasonal influenza vaccinations must take assignment on the claim for the vaccine. Shade Circles like this Not like this.
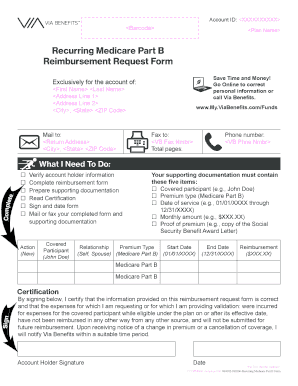 Recurring Medicare Part B Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
Recurring Medicare Part B Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
 Health Insurance Claim Forms Cms 1500 2 Part Continuation Package Of 1400 2012 U S Government Bookstore
Health Insurance Claim Forms Cms 1500 2 Part Continuation Package Of 1400 2012 U S Government Bookstore
Https Www1 Nyc Gov Assets Olr Downloads Pdf Health Med B Differential Form Pdf
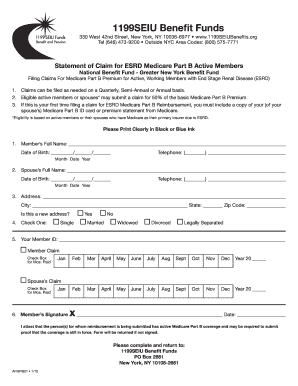
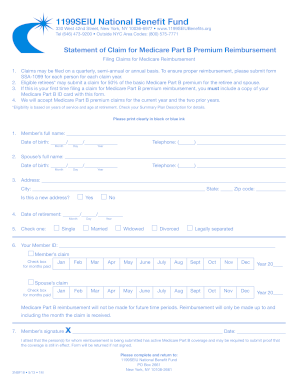
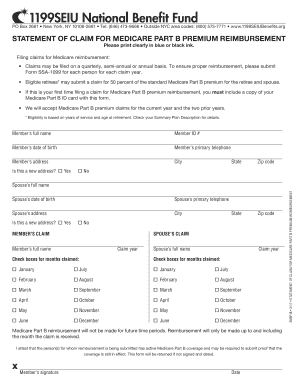 1199 Medicare Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
1199 Medicare Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
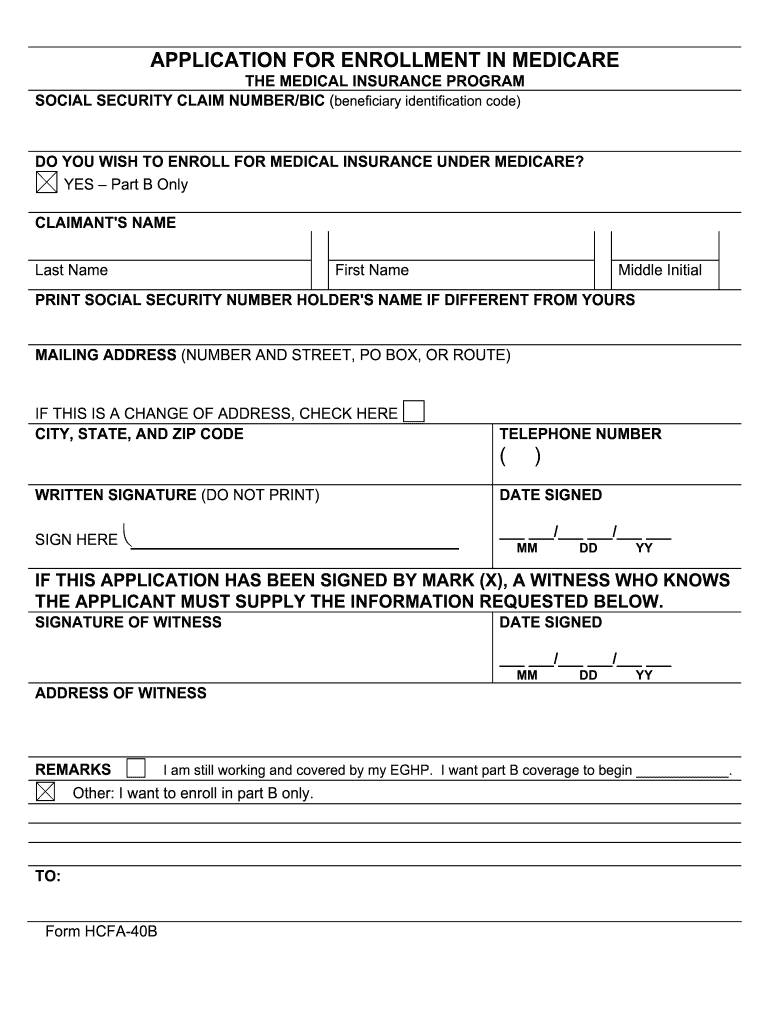 Form 40b Fill Online Printable Fillable Blank Pdffiller
Form 40b Fill Online Printable Fillable Blank Pdffiller
 Free 10 Sample Medicare Forms In Pdf Ms Word
Free 10 Sample Medicare Forms In Pdf Ms Word
 Medicare Part B Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
Medicare Part B Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
Medicare Part B Forms Printable Fill Online Printable Fillable Blank Pdffiller
 1199 Medicare Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
1199 Medicare Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
 B Reimbursement Fill Out And Sign Printable Pdf Template Signnow
B Reimbursement Fill Out And Sign Printable Pdf Template Signnow
Https Ngsmedicare Com Ngs Wcm Connect Ngsmedicare 2843d5e1 40b5 45f3 8b18 159227b66d32 1939 072519 B Reopening Request 508 Pdf Mod Ajperes Cvid Mn9osy7
 Medicare Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
Medicare Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
 Claim Form Tutorial Je Part B Noridian
Claim Form Tutorial Je Part B Noridian



No comments:
Post a Comment
Note: Only a member of this blog may post a comment.