To file a claim for those out-of-network services youll need to use the claim form from the state where you were treated. Download the health benefits claim form.
Http Louisville Edu Hr Forms Anthem Major Medical Claim
If you will be using electronic assistive devices to complete.

Bcbs out of network claim form. Click below to complete an electronic claim form. Form to Blue View Vision within one 1 year from the original date of service by the out-of-network providers office. As you complete the form youll want to have your member ID card and the itemized statement from your provider handy.
If youre a Blue Care Network member you can use the Member Reimbursement Form PDF to ask us to pay you back for medical services. Form To refer a patient who is a BlueCross BlueShield member to our disease management case management or health coaching service complete and fax this form to the number enclosed. Complete and return the.
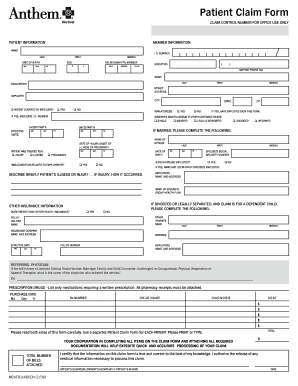
Vaccine Claim Form. Prescription Drug Prescription Drug Claim Form. Box 8504 Mason OH 45040-7111.
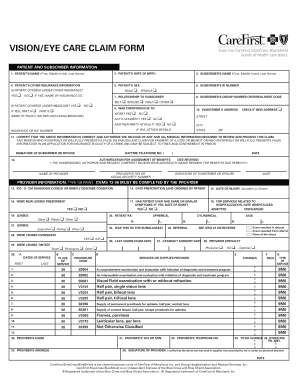
Vision Benefits Claim Form - Columbia Service Center Vision Benefits Claim Form - Greenville Service Center Healthy Vision Out-of-Network Claim Form. Blue View Vision will reimburse you for authorized services according to your plan design. Member Submitted Claim Form PDF File.
Bills should include the following information. To request reimbursement please complete and sign the itemized claim form. First American Administrators Inc.
Start by checking your benefit book to see if you have out-of-network coverage. Medicaid Claims Inquiry or Dispute Request Form. Out-of-network claim form its important that Blue Cross Blue Shield of Arizona BCBSAZ receives key pieces of information from you to process your claim.
Please complete the information below if the provider or services rendered were out of the United States. Section 1 Patient Information Section 2 Alternate Payee Information. RememberThis claim form should only be used when you see an Out-Of-Network provider who does not submit a claim for you.
For your claim to be processed we need to get key pieces of information from you. If yours does youll save money at the point of purchase when you use a network. If you go to an out-of-state doctor or hospital that doesnt participate with Blue Cross Blue Shield you may pay upfront for services.
Box 35 Durham NC 27702. For example you have to see an out-of-network doctor who doesnt accept your insurance. Form Title Networks Expedited Pre-service Clinical Appeal Form.
Blue Dental Out-Of-Network Claim Form PDF File. Birth Date MMDDYYYY Street Address City State. When visiting an out-of-network provider you are responsible for payment of services andor materials at the time of service.
Use this form to submit a health benefit claim for services that are covered under the Blue Cross and Blue Shield Service Benefit Plan. Name address and telephone number on official bill head of the PROVIDER rendering the service or supplying the item. English Version PDF File.
If your plan includes coverage for vision services you may need one of these forms to file your claims. Many of our plans include pharmacy and prescription drug benefits. Nonparticipating providers use this form to initiate a negotiation with Horizon BCBSNJ for allowed chargesamounts related to an inadvertent or involuntary service per the NJ Out-of-Network Consumer Protection Transparency Cost Containment and Accountability Act.
Medicaid only BCCHP and MMAI. Submit a separate claim for each patient. Green and get paid faster.
Out-of-network benefits your next step is to send us your completed claim form. Appeal Form PDF File. Please complete this section if someone other than the cardholder is to be reimbursed.
If you use a provider outside of our network youll need to complete and file a claim form to be reimbursed. Check the state-by-state list of Blue Cross Blue Shield companies to get started. You can submit your claim any time during the year.
Overseas members should use the Overseas Medical Claim Form. OUT-OF-NETWORK VISION SERVICES CLAIM FORM. Use a separate claim form for each family member and each physician or supplier.
If you choose an out-of-network provider please complete the following steps prior to submitting the claim form to EyeMed. Return the completed form and your itemized paid receipts to. Medicaid only BCCHP and MMAI Medicaid Service Authorization Dispute Resolution Request Form.
This form is only needed to submit claims for services and supplies that are not submitted by your provider ie out-of-network doctors and hospitals. Blue Dental Extra Dental Cleaning Enrollment Form PDF File If your plan offers a 3rd annual cleaning and you are pregnant or have diabetes you can use this form. Blue Cross and Blue Shield of North Carolina.
Submitting Form Information MAIL THIS FORM ITEMIZED RECEIPTS AND EXPLANATION OF BENEFITS if applicable TO. You can now submit your form online or by mail. Even when you have health insurance there may be occasions when you have to pay for services yourself.
Attach all itemized bills to this claim form. If you use a provider outside of the network you will need to complete and file a claim form for reimbursement. These contracting providers will file a claim on your behalf.
We know that filling out insurance forms. You must file your claim within one year from the date of service. Blue Cross Blue Shield Global Claim Form.
Spanish Version PDF File. Out of Plan Referral Review Request Form This form is used to request an Out-of-Plan Referral also referred to as an Out-of-Network. Claim Form This form does not need to be completed if your services were provided by a contracting hospital physician or dentist.
Not all plans have out-of-network benefits so please consult your member benefits information to ensure coverage of services andor materials from non-participating providers. Health Benefits Claim Form. If you do then download the out-of-network claim form.
 24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
Https Member Carefirst Com Carefirst Resources Pdf Health Benefits Claim Form In Service Area Cut0165 I Pdf
 24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 Empire Bcbs Claim Fill Online Printable Fillable Blank Pdffiller
Empire Bcbs Claim Fill Online Printable Fillable Blank Pdffiller
 Rx Group Number Bcbsmrx1 Reimbursement Form Blue Cross
Rx Group Number Bcbsmrx1 Reimbursement Form Blue Cross
Blue Cross Blue Shield International Medical Claim Form Pdfsimpli
 19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
Https Www Bcbstx Com Pdf Ut Medical Claim Form Pdf
 Blue Cross Blue Shield Claim Form Fill Online Printable Fillable Blank Pdffiller
Blue Cross Blue Shield Claim Form Fill Online Printable Fillable Blank Pdffiller
 24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
Https Provider Bluecrossma Com Providerhome Wcm Connect 8965a92a 1150 4ad1 Bb2b B34263f7c322 Mpc 031016 1x F Managed Care Out Of Network Request Form Pdf Mod Ajperes Convert To Url Cacheid 8965a92a 1150 4ad1 Bb2b B34263f7c322
Https Www Arkansasbluecross Com Docs Librariesprovider9 Default Document Library Medical Claim Form Ocr 508 Pdf Sfvrsn B4756efd 4
 19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
Https Www Bcbsil Com Pdf Forms Anc Oon Vis Serv Claim Il Pdf



No comments:
Post a Comment
Note: Only a member of this blog may post a comment.