ProviderGroup Name Provider Tax ID Number Provider NPI Number Provider County Date of Service Date of Last EOP Member Name Member ID Number Claim Number. If you wish to submit an appeal on behalf of a Healthy Blue member the member must first sign an Appeal Representative Form notifying Healthy Blue of their consent for you to represent him or her in the appeal process.
Https Selecthealth Org Plans Medicaid Media 86ed6c2201bd4d73b18d9bc3085fba15 Ashx
We or one of our providers refuse to give you a service you think should be covered.
Select health appeal form for providers. Incomplete appeal submissions will be returned unprocessed. By signing this form you agree to not bill the member for the services that have been denied. Attach the claim form and all supporting documentation please check Provider Manual at.
Request for Medicare Prescription Drug Coverage Determination Form Use this form to request a Medicare Advantage Part D Drug. Complete the online fillable form and save it to your computerdevice see below. Medicare Advantage Waiver of Liability Noncontracted providers who have had a Medicare claim denied for payment and want to appeal must submit a signed Waiver of Liability Form to us.
Provider Claim Dispute Form. HOW WOULD YOU LIKE US TO CONTACT YOU ABOUT THIS APPEAL. Mail or fax the form to SelectHealth within 60 days from the date the claim was processed to.
Find change forms for every scenario. APPEALRECONSIDERATION REQUEST FORM SIGNATURE Please attach copies of any records such as bills or letters from doctors and send them by email fax or mail. Member consent for provider to file an appeal PDF Newborn prior authorization form PDF Pregnancy risk assessment form PDF Prior authorization form general PDF PTOTSTChiro request for authorization PDF Universal 17P authorization form PDF Pharmacy authorization forms.
Oral Appeals must be followed by a written signed Appeal. Appeals must be requested no less than 60 calendar days of the date on the Initial Adverse Determination. Provider Information Form Update your records electronically or by mailing a completed form.
Physician request form for hepatitis C therapies PDF. A provider may file an appeal on behalf of a Healthy Blue member but only with the members written consent. Mail the completed form to the following address.
If you have a complaint we want to know. THE PROVIDER ANDOR REVIEW MY RECORDS. Call us at 855-442-9900.
Please let us know how we can help. Home Care Services Authorization for MHCP PDF National Provider Identifier. We or one of our plan providers reduces or cuts back on a service you have been receiving.
This includes but is not limited to permitting SWH access to member treatment. Signature Date Subscriber or Patient PO. SWHs expectation is that each provider will fully cooperate and participate with its fraud waste and abuse programs.
The PAR Form is used for all provider inquiries and appeals related to reimbursement. For specific appeal guidelines to the completed HPI Provider Appeal Form ie. An appeal may be filed by the member or his or her designee orally or in writing.
Out-of-Network RAPL Payment Appeal Form PDF Missouri Out-of-Network Appeal Form PDF Nebraska Out-of-Network Appeal Form PDF Payment Resources for EOBPRA835 Cosmos Platform PRA PDF Provider Remittance Advice. Providers license or the loss of any certification or permit by any federal authority or by any state in which the provider is authorized to provide healthcare services Cooperate with SWH audits and reviews. Providers may request corrective adjustments to any previous payment using this form.
Complete all information required on the Provider Appeal Form. Download the Provider Appeal form. P Health Net Commercial Provider Appeals Unit PO Box 9040 Farmington MO 63640-9040 Commercial Provider Services Center 1-800-641-7761 Health Net Medi-Cal Provider Appeals Unit OBox 989881 West Sacrament CA 95798-9881.
Provider Appeal Form Date Provider Name Office Contact Address City State ZIP Telephone Fax Patient Name Subscriber ID Date of Service Billed Amount SelectHealth Claim Auth Claim denial reason. If you need to make a change to your SelectHealth plan theres a form for that. I UNDERSTAND THAT SELECTHEALTH MAY NEED TO CONTACT THE PROVIDER.
Program Integrity Audit Reconsideration and Appeals Policy. Please note the speciic address for all Medi-Cal appeals. Is defined as a request from a health care provider to change a decision made by Select Health of South Carolina related to claim payment or denial for services already provided.
To request reconsideration of a service or decision you have the right to file an appeal or grievance. Member Name Claim Appeal Submission Date Member ID Date of Service Provider Name Providers Office Contact Name Provider Telephone Please note the following in order to avoid delays in processing provider appeals. A disagreement with the nonpayment denial or reduction of a covered service rendered out of the network including emergency care.
You think we are stopping your coverage for a service too soon. Filing a formal appeal. NPI Submission Form PDF Out-of-Network Appeal Forms.
Provider appeals filing limit policy. Pharmacy prior authorization form. WHAT IS THE REASON FOR YOUR APPEAL.
A provider dispute is not a pre-service appeal of a denied or reduced authorization for services or an administrative complaint. Wed love to make it right. This form must be used to file your dispute.
Address as shown above I GIVE SELECTHEALTH PERMISSION TO LOOK INTO MY APPEAL. WHAT WOULD YOU LIKE US TO DO.
Https Selecthealth Org Media Selecthealth Medicare Pdf Misc Grievance Form Ashx
 Member Appeals
Member Appeals
 Member Appeals
Member Appeals
Https Selecthealth Org Medicare Member Care Media 058d087007304a1cb40eb317d06059f8 Ashx
 Member Appeals
Member Appeals
Https Www Selecthealthofsc Com Pdf Provider Resources Provider Claim Dispute Form Pdf
Https Www Firstchoicevipcareplus Com Assets Pdf Provider Claim Inquiry Form Pdf
Https Www Umpquahealth Com Wp Content Uploads 2020 04 Claims Appeal Reconsideration Form Fillable 4 10 2020 Pdf
Https Www Hopkinsmedicine Org Johns Hopkins Healthcare Downloads All Plans Claims And Payment Disputes Pdf
Https Www Aetnabetterhealth Com Illinois Assets Pdf Providers Il 20non Par 20provider 20appeal 20form Pdf
 Provider Appeals
Provider Appeals
Https Www Selecthealthofsc Com Pdf Provider Billing Inquiry Dispute Appeal Ref Guide Pdf
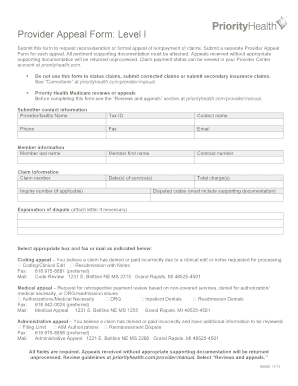
Priority Health Appeal Form Fill Online Printable Fillable Blank Pdffiller
Https Selecthealth Org Media Selecthealth82 Pdf Documents Forms 4101 Appeal Form Ff A Ashx



No comments:
Post a Comment
Note: Only a member of this blog may post a comment.