Blue Cross Blue Shield of Massachusetts will make a reimbursement decision within 30 calendar days of receiving a completed request form. Click on Claim Forms and choose the form preferred For more information and to confirm your coverage please call Customer Service.
Https Www Bcbstx Com Pdf Ut Medical Claim Form Pdf
Receive reimbursement funds via direct deposit.

Bcbs reimbursement form. Request for Reimbursement. Blue Shield BCBS members utilizing claim forms as set forth in The Billing and Reimbursement section of this manual. Youll go to a page that explains the form and has a link to download it.
Please ensure your supporting documentation clearly indicates the requested amount. Do not attach a balance forward bill Patients full name. I certify that the information on this form is accurate and complete.
English Health Benefits Election Form SF 2809 Form. Prescription Drug Claim Form Members with pharmacy benefits through BCBSTX can use this form to request reimbursement for a prescription drug purchase. Reimbursement may be considered taxable income so consult your tax advisor.
You can use these claim forms to ask us for reimbursement. If you take advantage of Service Benefit Plan dental benefits you will need to complete and file a claim form for reimbursement. For vision reimbursement claims through 123120 please submit to EyeMed.
Attach the bill or clear copy of the bill to this form. Fill out the Medical Expense Claim form include all requested information. Just choose the form based on your group or plan and the service.
In-network providers will need to enter a password to access this section of the site. If you were on a cruise youll use the same claim form for reimbursement. Receive reimbursement funds via mailed check.
Date of treatment. I have notwill not seek reimbursement of this expense from any other plan or party because I. Check the appropriate box in Supporting Documentation section and attach Acceptable Supporting Documentation as described below.
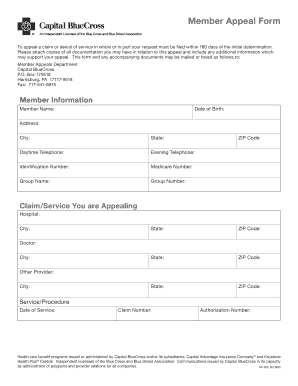
Form Title Networks Expedited Pre-service Clinical Appeal Form. This section provides additional reimbursement details. Employee must complete.
We process most claims within 10 days of receipt. Medicaid only BCCHP and MMAI Medicaid Service Authorization Dispute Resolution Request Form. Accept the terms and conditions.
Fax copies of receipts proof of premium payment along with your form to 877-353-9236. Medicaid only BCCHP and MMAI. If youre a Blue Care Network member you can use the Member Reimbursement Form PDF to ask us to pay you back for medical services.
I am requesting reimbursement for Medicare Part B premium expenses I incurred while a member of the Blue Cross and Blue Shield Service Benefit Plan. Health Care Services Referral Form To refer a patient who is a BlueCross BlueShield member to our disease management case management or health coaching service complete and fax this form to the number enclosed. Blue Cross Blue Shield of Massachusetts will make a reimbursement decision within 30 calendar days of receiving a completed request form.
Reimbursement may be considered taxable income so consult your tax advisor. Your bill should include the following information. Reimbursement requests must be received by Blue Cross Blue Shield of Rhode Island no later.
Blue Essentials SM Blue Advantage HMO SM and Blue Premier SM. Complete this form if you are visiting a provider that is not a participating provider in the EyeMed network. Medicaid Claims Inquiry or Dispute Request Form.
Browse commonly requested forms to find and download the one you need for various topics including pharmacy enrollment claims and more. If youre in a religiously accommodated group and you paid for your own contraceptive prescription or service you can get reimbursed using the Contraceptive Accommodation Choice Enrollment Form. Follow the steps below to access the claim form.
Sometimes the form is called Member Application for Payment Consideration which is the same as a claim form. For reimbursement submit the Wellness Reimbursement form on the opposite side along with proof of payment to the address shown below. Reimbursement is sent to the members address on file with Blue Cross.
The original pharmacy receipt must be submitted with the completed form to Prime Therapeutics the. Reimbursement is sent to the members address on file with Blue Cross. Reimbursement is sent to the members address on file with Blue Cross.
Use this form to request reimbursement for services received from providers who do not participate in the Davis Vision network. Enter the 3 character prefix from the members ID. Blue Cross Blue Shield of Massachusetts will make a reimbursement decision within 30 calendar days of receiving a completed request form.
In addition to the instructions in this section and other sections of the manual participating providers Provider shall adhere to the following policies with respect to filing claims for Covered Services to BCBS members. EyeMed Vision Services Claim Form. Member Reimbursement Donor Egg and Sperm.
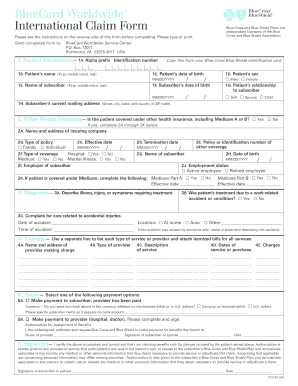
 Download Blue Cross Blue Shield International Medical Claim Form For Free Formtemplate
Download Blue Cross Blue Shield International Medical Claim Form For Free Formtemplate
 19 Printable Blue Cross Blue Shield Reimbursement Forms Templates Fillable Samples In Pdf Word To Download Pdffiller
19 Printable Blue Cross Blue Shield Reimbursement Forms Templates Fillable Samples In Pdf Word To Download Pdffiller
 Blue Cross Blue Shield Overseas Medical Claim Form Fill Out And Sign Printable Pdf Template Signnow
Blue Cross Blue Shield Overseas Medical Claim Form Fill Out And Sign Printable Pdf Template Signnow
 19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
 Blue Cross Blue Shield Claim Form Fill Online Printable Fillable Blank Pdffiller
Blue Cross Blue Shield Claim Form Fill Online Printable Fillable Blank Pdffiller
 21 Printable Blue Cross Blue Shield Health Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
21 Printable Blue Cross Blue Shield Health Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 Blue Cross Blue Shield International Medical Claim Form Pdfsimpli
Blue Cross Blue Shield International Medical Claim Form Pdfsimpli
 Blue Cross Blue Shield International Fillable Claim Form Fill Online Printable Fillable Blank Pdffiller
Blue Cross Blue Shield International Fillable Claim Form Fill Online Printable Fillable Blank Pdffiller
24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
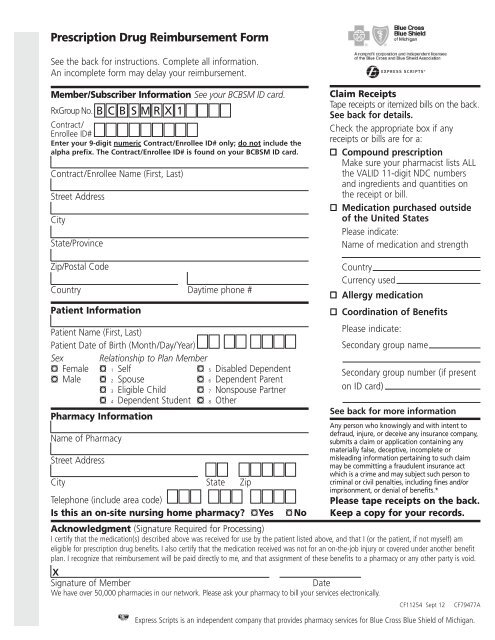 Rx Group Number Bcbsmrx1 Reimbursement Form Blue Cross
Rx Group Number Bcbsmrx1 Reimbursement Form Blue Cross
 24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
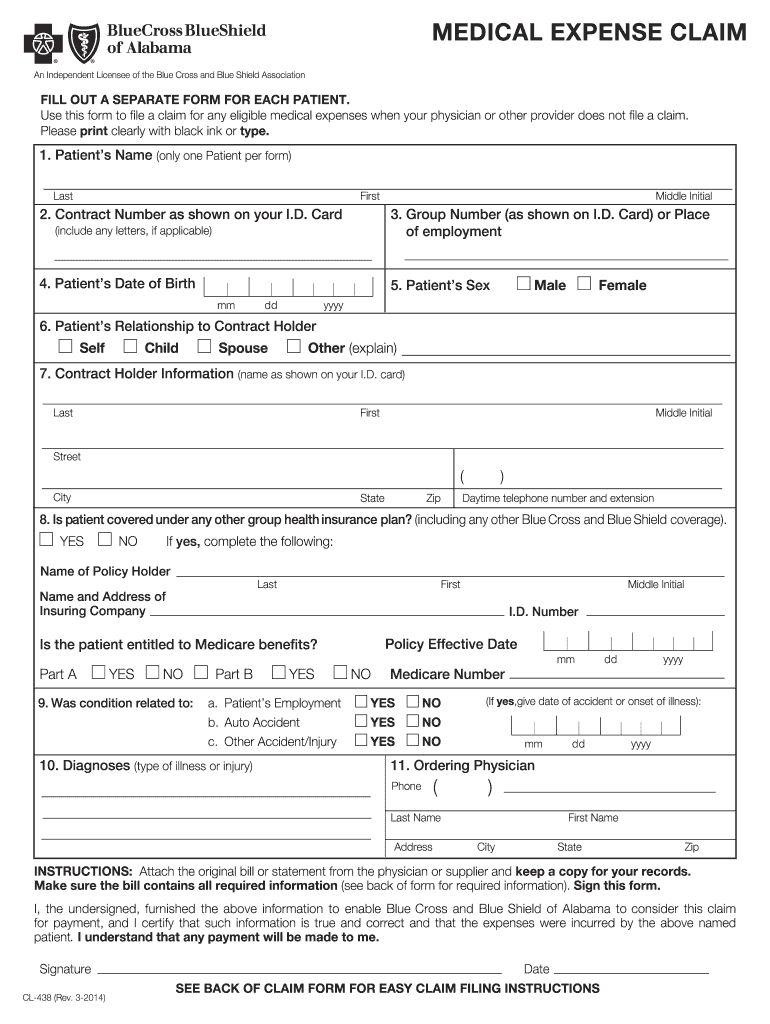 Blue Cross Blue Shield Of Alabama Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
Blue Cross Blue Shield Of Alabama Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
 24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller



No comments:
Post a Comment
Note: Only a member of this blog may post a comment.